When roles are approved in behavioral health organizations, they’re often not fully funded. This creates a gap between what’s planned and what’s financially sustainable. Key issues include:
- Budgeted vs. Funded Roles: Approved roles may lack reliable financial backing, leading to hiring freezes or rescinded offers.
- Funding Challenges: Medicaid reimbursement rates often fall short, and grants rarely cover overhead costs like IT or supervision.
- HR vs. Finance Disconnect: HR focuses on filling roles, while Finance prioritizes cost control, causing misaligned decisions.
- Reimbursement Models: Fee-for-Service (FFS) funding limits non-billable activities, while contract-based models offer stability but shift financial risk to providers.
- Turnover Impact: Underfunded roles lead to burnout, high turnover, and reduced care quality, costing organizations time and money.
Solution: Tools like DATIS integrate HR and Finance systems, ensuring roles are tied to actual funding sources. This prevents hiring errors, aligns staffing with budgets, and supports financial stability.
Budgeted vs. Funded: What’s the Difference?
A budgeted role refers to a position that’s been approved in an organization’s annual plan or service budget. Essentially, it’s a spot that appears in headcount projections and staffing plans. On the other hand, a funded role is one that has actual, reliable financial backing – whether through verified reimbursement rates, active grants, or confirmed financial allocations. This funding ensures the organization can cover all costs associated with hiring and retaining someone in that role.
In behavioral health, the gap between budgeted and funded roles is a frequent issue. While a position might be budgeted based on service demands, it often lacks the sustainable revenue needed to make it viable. For example, if Medicaid reimbursement rates fall short of covering competitive market wages, the role becomes unfunded in practice. This makes it financially unsustainable without causing losses.
And it’s not just about salaries. Grants and waivers might cover base wages but rarely account for other critical overhead costs – billing systems, IT infrastructure, clinical supervision, compliance expenses, and more. As a result, even a “funded” role can become a financial strain before hiring even begins.
Why Finance and HR Don’t Always Align
Human Resources (HR) and Finance departments often work toward different goals, which can create friction. HR focuses on headcount and filling vacancies to meet operational needs. Meanwhile, Finance prioritizes labor expenses and cash flow, ensuring payroll obligations can be met both now and in the future. This divergence can lead to situations where a role is approved in theory but isn’t supported by the revenue required to sustain it.
This disconnect is especially problematic in behavioral health, where funding is often unstable. Grants are time-limited, and Medicaid reimbursement rates can fluctuate. As a result, a role might remain “budgeted” on paper, but its funding status could change mid-year. This leaves organizations in difficult positions – posting jobs they can’t afford to fill or, even worse, rescinding offers when funding falls through.
Behavioral Health Funding Challenges
Behavioral health providers face unique financial challenges, which amplify these funding mismatches. Medicaid is a primary source of revenue, but its reimbursement rates are notoriously low. Unlike primary care, behavioral health services don’t benefit from federal technology incentives, limiting access to capital for tracking funding in real time.
“Every single service provided to a person with a mental illness or addiction treatment disorder in the Medicaid program is optional”.
When federal or state budgets get tight, behavioral health services – like rehabilitation, case management, and clinic options – are often the first to face cuts. For instance, in March 2025, the federal administration terminated $1.3 billion in unspent Mental Health and Substance Abuse Prevention and Treatment Block Grant funds. Just months later, in July 2025, the passage of H.R.1 reduced federal Medicaid funding by 15%. This reduction is projected to leave 11.8 million Americans without coverage. When grants dry up or reimbursement rates drop, organizations are left with staffing plans they can’t afford to implement.
Contract vs. Fee-for-Service: How Reimbursement Models Affect Funding
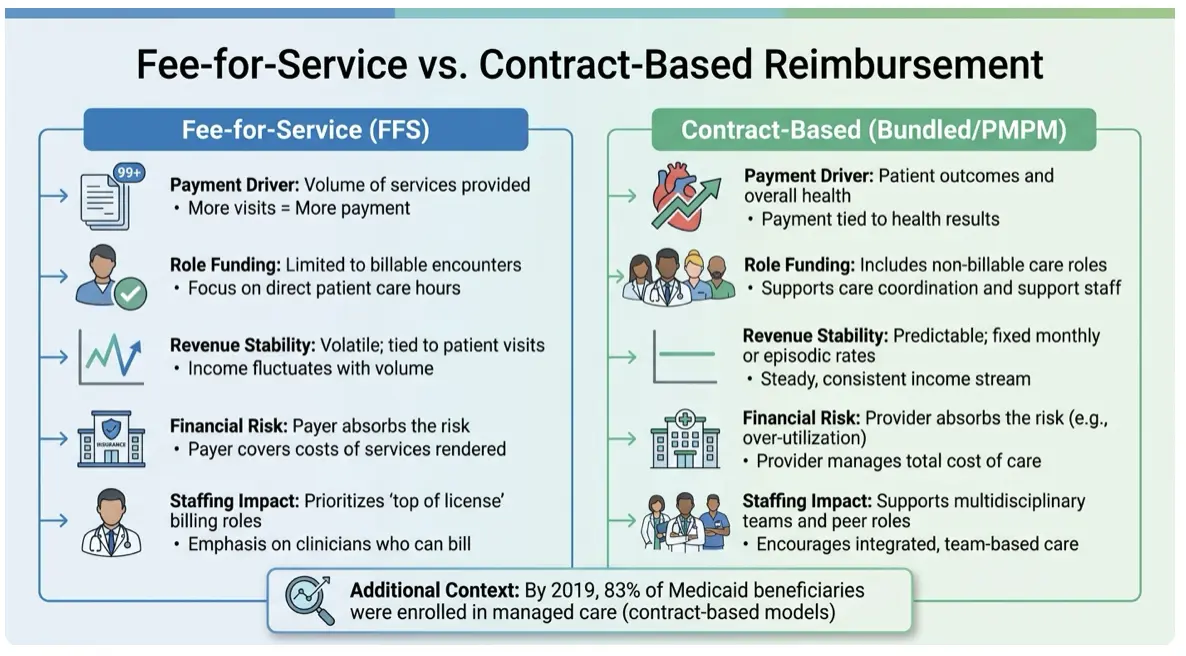
Approved roles might look funded on paper, but reimbursement models often tell a different story.
Payment structures play a big role in determining which positions are financially sustainable. Take Fee-for-Service (FFS), for example – it only reimburses for direct patient interactions. This creates a gap for activities like care coordination calls, team meetings, patient outreach, or documentation. These are essential tasks that happen daily, yet they don’t generate revenue under traditional FFS models.
On the other hand, contract-based models – such as Per Member Per Month (PMPM) or bundled payments – offer a fixed payment regardless of the number of appointments. This approach funds critical non-billable roles, making positions like peer support specialists, care managers, and vocational specialists financially feasible. Since revenue isn’t tied to individual billable encounters, these roles become more viable. By 2019, 83% of Medicaid beneficiaries were enrolled in managed care, reflecting a shift toward these models.
However, contract-based models come with their own challenges. Providers bear the financial risk when care costs exceed the fixed payment, especially during high-resource phases like early treatment. For instance, Mobile Crisis Teams face a tough dilemma under FFS – they must maintain 24/7 staffing but only get reimbursed for active service calls, not for on-call hours or travel time.
Contract vs. Fee-for-Service: A Comparison
|
Feature |
Fee-for-Service (FFS) |
Contract-Based (Bundled/PMPM) |
|
Payment Driver |
Volume of services provided |
Patient outcomes and overall health |
|
Role Funding |
Limited to billable encounters |
Includes non-billable care roles |
|
Revenue Stability |
Volatile; tied to patient visits |
Predictable; fixed monthly or episodic rates |
|
Financial Risk |
Payer absorbs the risk |
Provider absorbs the risk (e.g., over-utilization) |
|
Staffing Impact |
Prioritizes “top of license” billing roles |
Supports multidisciplinary teams and peer roles |
It’s worth noting that funding viability also depends on the payer. For example, a role might be covered under Medicaid but not by Medicare or private insurance.
How CMS Value-Based Care Policies Complicate Funding
The Centers for Medicare & Medicaid Services (CMS) aims to link 100% of Medicare beneficiaries to value-based care models by 2030. While this shift is promising, it adds new challenges for workforce funding.
CMS introduced Psychiatric Collaborative Care Model (CoCM) billing codes to support behavioral health coordination – tasks that were previously unbillable. These codes allow primary care providers to bill for psychiatric consultations and care management activities. Yet, adoption has been slow. Why? The documentation requirements are heavy, and organizations need specialized health IT systems to manage registry data and track care engagement. As of 2018, only 37 states covered peer support services through Medicaid state plans or waivers.
The transition to value-based care forces organizations to juggle two systems: traditional volume-based reimbursement and newer quality-based payments. This dual structure complicates cash flow and makes it harder to determine whether a role is truly funded or just appears sustainable on paper.
What Happens When Funding and Roles Don’t Match
When funding falls short of covering approved roles, behavioral health organizations face serious financial and workforce challenges. These mismatches disrupt operations, making it harder to deliver care effectively.
Financial Problems from Unfunded Roles
Unfunded roles create ripple effects across an organization’s finances. When reimbursement rates don’t align with labor market demands, vacancies lead to lost revenue. The gap between the cost of positions and actual reimbursement becomes a constant strain on budgets.
The situation worsens when claims for behavioral health services are denied – a common issue, as mental health claims are rejected at twice the rate of physical health claims. Each denial represents unpaid work, which drains cash flow, especially when budgets are based on overly optimistic revenue projections.
This financial instability is part of a larger issue. Behavioral health care is often underfunded, with insurance reimbursements for mental health visits averaging 22% less than those for medical or surgical visits. Federal policy changes have also had a huge impact. For example, H.R. 1, passed in July 2025, slashed federal Medicaid funding by 15%, amounting to a $1 trillion cut over a decade. Additionally, the federal government clawed back over $1.3 billion in unspent mental health and substance use block grants, leaving organizations scrambling to cover roles that were previously funded.
Real-world examples highlight the consequences of these funding gaps. In January 2026, the Shawnee Police Department in Oklahoma lost a federal grant for a crisis intervention team, forcing a shift from treatment referrals to increased arrests and fewer suicide response resources. Similarly, Covington County, Alabama, had to shut down a program pairing deputies with mental health professionals, leaving law enforcement to handle mental health calls without specialized help.
These funding disruptions don’t just impact payroll – they also complicate compliance with reporting requirements tied to various funding streams. Without accurate data, leadership is left making decisions based on assumptions, which can jeopardize future funding. The result? A cycle of financial strain that undermines both operations and workforce stability.
How Funding Gaps Affect Turnover and Morale
Funding shortfalls don’t just hurt the bottom line – they also take a toll on staff morale and retention. When roles are underfunded, the workload shifts to existing employees, leading to burnout and increased turnover.
The costs of turnover are staggering. Replacing a leader or manager can cost up to 200% of their annual salary, while technical professionals cost about 80%, and frontline employees around 40%. On top of that, the hiring process often takes six to nine months of an employee’s salary. Alarmingly, 42% of employees who leave voluntarily say their departure could have been prevented, with 30% citing compensation or benefits and 9% pointing to staffing or workload issues. When organizations can’t offer competitive wages or maintain adequate staffing, they risk falling into a turnover crisis.
This staffing instability creates a snowball effect. Overworked teams deliver a lower quality of care, leading to more claim denials, longer wait times, and tighter margins. These challenges make it even harder to attract new talent, reinforcing a reputation for high turnover and further complicating recruitment efforts. Currently, 51% of U.S. employees are either actively job-hunting or open to new opportunities, leaving organizations with funding gaps especially vulnerable.
The broader impact is enormous. U.S. businesses lose up to $1.8 trillion annually due to poor employee experiences and turnover. For behavioral health organizations already operating on thin margins, this poses a serious threat. Managing fragmented systems to align staffing and funding diverts attention from their mission – precisely when mission-driven work is needed most to retain dedicated employees. DATIS addresses this challenge by integrating HR and finance systems, offering clear visibility into workforce costs and revenue alignment to prevent funding gaps.
How DATIS Connects HR and Finance for Better Funding Visibility
The disconnect between HR approvals and actual funding doesn’t have to be a constant struggle. DATIS bridges this gap by integrating HR, payroll, and finance data into one unified platform. By moving away from spreadsheets and manual coordination, behavioral health organizations gain real-time visibility into whether each role is genuinely supported by available funds. This streamlined approach directly tackles the funding gaps mentioned earlier, enabling precise role planning, funding verification, and cost tracking.
Connecting Role Planning to Revenue Forecasts
DATIS employs a position-control architecture instead of relying on an employee-centric model. Here’s how it works: every role is treated as an individual budget line tied to its funding source, such as a Medicaid contract, federal grant, or fee-for-service revenue. If a grant is nearing expiration or a contract underperforms, leadership can immediately identify which positions might be affected. This allows them to adjust hiring plans before resources are committed.
This system shifts workforce planning from being reactive to proactive. Organizations can align workforce strategies with revenue forecasts in advance. For instance, if a program isn’t delivering the expected reimbursements, the platform pinpoints the at-risk positions. This ensures CFOs and HR leaders are making decisions based on the same up-to-date data, avoiding conflicting assumptions.
Verifying Funding Before Hiring
With Position Control, the system acts as a safeguard to prevent unfunded hires. Before posting a job or extending an offer, DATIS automatically verifies if funding is available. This eliminates the risk of hiring based on outdated approvals.
The platform also ensures that labor costs are allocated correctly across programs, grants, or cost centers. This is especially critical for behavioral health organizations managing a variety of funding streams. Marion McLaurin, Senior VP of Human Resources, underscores this point:
“If you’re in Health and Human Services, then this is the product. This is the way to go. Because they’ve already designed it according to that industry, and it just makes sense”.
Tracking Workforce Costs Against Outcomes
DATIS goes beyond initial funding checks by aligning workforce costs with service outcomes, ensuring ongoing financial accountability.
The platform links staffing costs directly to service delivery and outcomes, which supports both compliance and financial oversight. By tracking labor hours against service codes, organizations can accurately calculate delivery costs – a crucial capability for transitioning to value-based care models and meeting CMS reporting requirements.
DATIS’s Business Intelligence and Analytics tools turn workforce data into actionable insights. Executives can monitor how labor costs – which often account for 70-80% of an organization’s budget – affect financial performance in real time. Brian Kennedy, General Manager of DATIS, highlights this advantage:
“If you have complicated funding streams that require you to report information back to them… then there is not another tool on the market that can do for you what the e3 product can do for you”.
This level of transparency helps organizations determine which programs are financially viable and which may need adjustments – well before funding issues lead to turnover or service disruptions.
Conclusion: Matching Workforce Plans to Financial Reality
When roles are approved without confirming funding, it can disrupt growth and lead to unexpected hiring freezes. Behavioral health organizations that fail to differentiate between authorized headcount (positions approved in an HR system) and funded headcount (positions backed by actual budget allocations) risk facing workforce restructuring, overspending, and compliance challenges.
DATIS bridges this gap by integrating HR and finance for seamless workforce planning. Its Position Control framework ensures every job is tied to a funding source – whether that funding comes from Medicaid contracts, federal grants, or fee-for-service revenue streams.
For leaders in behavioral health, this means fewer surprises and smarter decisions. Instead of discovering funding shortfalls after making job offers, organizations can confirm funding in advance. CFOs also gain the ability to monitor turnover as a measurable financial risk.
Shifting from reactive problem-solving to proactive planning allows organizations to treat workforce strategy as a continuous financial priority. When HR and finance collaborate effectively, staffing plans can focus on offering competitive wages to retain clinicians rather than relying on unsustainable hiring practices. This approach not only strengthens financial stability but also supports staff morale by ensuring proper supervision, reasonable caseloads, and balanced workloads.




{kind=link}
{kind=link}
{kind=link}