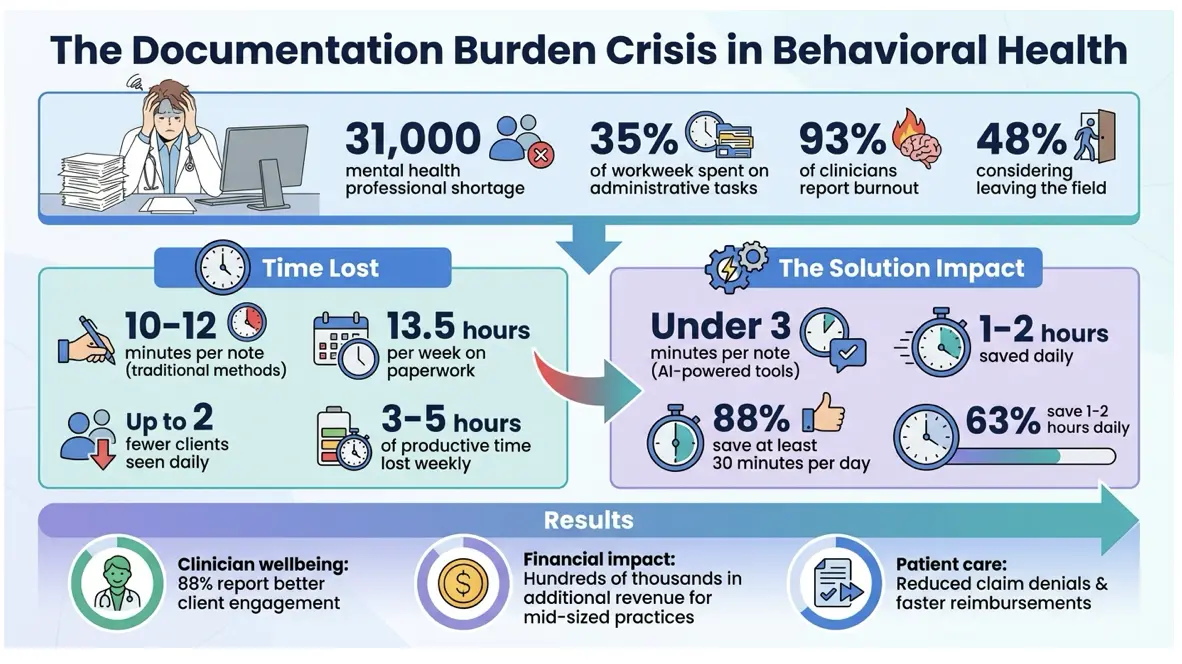
Behavioral health providers face increasing challenges: rising demand for services, a shortage of 31,000 mental health professionals, and administrative tasks consuming 35% of their workweek. Documentation inefficiencies lead to burnout, reduced productivity, and financial strain, with 93% of clinicians reporting burnout and 48% considering leaving the field. Ineffective electronic health record (EHR) systems designed for physical healthcare further complicate workflows, forcing manual data entry and increasing errors.
Key Takeaways:
- Clinicians lose time due to outdated documentation processes, seeing up to two fewer clients daily.
- Generic EHR systems lack features tailored for behavioral health, like group therapy workflows and compliance tools.
- AI-powered tools and behavioral health-specific software reduce note completion times from 10–12 minutes to under 3 minutes, saving 1–2 hours daily.
- Integrated systems align documentation with billing, reducing errors and speeding up reimbursements.
Efficient documentation tools improve clinician productivity, reduce burnout, and enhance patient care. By addressing these issues, organizations can better meet growing demand while supporting their staff and maintaining financial stability.
The Real Cost of Inefficient Documentation
The problems caused by poor documentation don’t just stop at limiting an organization’s capacity – they ripple out, affecting clinician well-being, operational workflows, and financial health across the board.
Clinician Burnout and Lower Productivity
When clinicians can’t finish their notes during work hours, the task often spills over into their personal time. This “after-hours documentation” means they’re logging in late at night or on weekends, blurring the line between work and personal life . For behavioral health clinicians, this shift from client care to repetitive paperwork takes a heavy toll. A staggering 77% report significant mental fatigue – the highest rate among all medical specialties – and this fatigue can lead to seeing up to two fewer clients per day .
Operational Challenges Across Departments
Inefficient documentation doesn’t just weigh on clinicians; it creates headaches across the entire organization. Compliance teams often have to step in when notes are incomplete or unclear, increasing their workload. Without tools that flag essential regulatory elements – like those required under HIPAA or 42 CFR Part 2 – organizations become more vulnerable to audits . On top of that, manual signature processes slow down the finalization of records and billing, creating unnecessary bottlenecks.
Group therapy programs face their own unique struggles. Many behavioral health EHR software systems are built for individual patient workflows, forcing clinicians to manually duplicate session notes for every participant. This redundancy not only wastes time but also raises the risk of privacy violations.
Revenue Delays and Service Limitations
These operational inefficiencies have a direct impact on an organization’s financial health. In many states, clinicians can’t bill for the time they spend on documentation, making it crucial to complete notes quickly and accurately. When notes are left unfinished, claim submissions get delayed, disrupting cash flow – especially at a time when many organizations are trying to scale up services to meet growing demand.
Incomplete or unclear documentation also increases the likelihood of denied or delayed reimbursements. Manual data entry into billing systems is another pain point – it’s time-consuming and prone to errors, leading to costly resubmissions. For medium-sized practices, clinicians working with inefficient systems can lose 3–5 hours of productive time each week. Over time, this adds up to hundreds of thousands of dollars in lost revenue. When administrative systems fail to support clinical workflows, it becomes nearly impossible for organizations to expand services, even when demand is surging.
Common Documentation Problems in Behavioral Health
Problems with Generic EHR Systems
Many EHR systems were never designed with behavioral health in mind – they were built for physical healthcare. This creates ongoing hurdles for behavioral health providers trying to adapt these systems to their needs.
One major issue is duplicate data entry, which eats up valuable time. For instance, in group therapy sessions, clinicians often have to manually re-enter the same details – such as the session’s date, time, and interventions – for each participant. Geetha Pradeep, Senior Content Specialist at blueBriX, highlights this problem:
“Most EHR systems were designed for one provider, one patient, one chart and not for six participants, shared interventions, and individualized notes”.
Additionally, these systems rely heavily on checkboxes and rigid templates. This approach doesn’t capture the depth of therapeutic insights, forcing clinicians to copy and paste notes, which can lead to compliance issues during audits.
Another critical gap is the lack of a “Golden Thread” – a seamless connection between treatment plans, progress notes, and outcomes. Without this, justifying billing becomes more difficult. When EHRs don’t integrate with billing systems, staff end up entering the same data multiple times, increasing the risk of costly errors.
These challenges emphasize how poorly generic EHRs align with the specific needs of behavioral health, underscoring the demand for specialized tools.
Why Physical Health EHRs Don’t Fit Behavioral Health
The shortcomings of generic EHR systems stem from their design, which is tailored for physical healthcare. These platforms operate on a “one provider, one patient, one record” model, making them unsuitable for behavioral health’s multi-client workflows. This design flaw also raises privacy concerns under HIPAA and 42 CFR Part 2.
Behavioral health providers face unique requirements, such as managing PHQ-9 scores, aligning with DSM-5 criteria, and adhering to 42 CFR Part 2 regulations. Generic systems often fail to support these needs.
Another issue is the high cost of context switching. Clinicians must shift their focus from providing care to navigating irrelevant medical fields and checkboxes, which disrupts both documentation quality and the therapeutic relationship. A study on integrated care practices found that 39% of psychiatrists resorted to keeping “off-system” notes because their EHRs were so poorly suited to their work.
This disconnect between system design and behavioral health needs not only increases the documentation burden but also detracts from the time and energy clinicians can devote to patient care.
How Behavioral Health-Specific Software Reduces Documentation Burden
Integrated Workflows Across Programs
Behavioral health-specific software simplifies documentation by linking treatment plans, goals, and outcomes directly to session notes. This eliminates the need for duplicate data entry across various programs, saving time and effort for clinicians.
For group therapy sessions, these platforms allow providers to create a master note that automatically fills in session details for all participants. At the same time, they support individualized progress notes for each patient. Additionally, these systems can calculate patient-reported outcomes, such as PHQ-9 and GAD-7 scores, and embed them directly into clinical notes. This feature is especially useful for tracking progress in Intensive Outpatient (IOP) and Partial Hospitalization (PHP) programs.
By combining integrated workflows with automation, these tools significantly reduce the need for manual data entry.
Using Automation and AI to Save Time
AI-powered tools, including ambient listening technology, take documentation a step further by capturing session details and instantly generating structured notes. This allows clinicians to stay fully engaged with their clients without being distracted by typing.
For example, Beacon Outpatient Management introduced Qualifacts iQ Clinical Documentation in early 2025. By November 2025, 30% of its 300 clinicians had adopted the tool, cutting the time needed to complete a note from 10–12 minutes to under 3 minutes. The organization plans to reach 75% adoption by Q1 2026 to further reduce documentation workloads.
Similarly, a January 2026 case study from InStride Health revealed that 63% of clinical evaluators saved one to two hours daily using AI scribe tools, while 88% saved at least 30 minutes per day. Four weeks after implementation, all evaluators continued to use the tool, underscoring its effectiveness.
These time-saving innovations also improve accuracy, paving the way for smoother billing processes.
Connecting Documentation to Billing
When documentation and billing systems are integrated, it significantly reduces revenue cycle delays. These platforms can suggest appropriate CPT and E/M codes based on session details and include built-in checks to catch documentation gaps or coding errors before claims are submitted. This reduces manual errors and minimizes claim denials.
Clinical notes are automatically linked to billing activities, eliminating repetitive data entry between departments. This ensures that claims can be submitted promptly after sessions are documented, allowing clinicians to spend less time on administrative tasks and more on patient care.
For organizations with multiple locations, this integration provides a consolidated view of revenue cycle performance across all sites, making it easier to identify and resolve billing issues efficiently.
Results: What Efficient Documentation Delivers
Better Clinician Productivity and Job Satisfaction
When clinicians spend less time on documentation, they can focus more on their primary goal: providing care. With the use of AI-powered documentation tools, note completion times have dropped significantly – from 10–12 minutes to under 3 minutes. In fact, studies reveal that 88% of clinical evaluators save at least 30 minutes daily, with 63% saving as much as 2 hours per day. Additionally, 88% of clinicians report better client engagement as a result.
Cutting down after-hours documentation also tackles burnout, a growing issue among behavioral health workers. With 93% experiencing burnout and nearly 48% considering leaving their jobs due to overwhelming workloads, streamlined documentation can make a big difference. It helps clinicians maintain the empathy and focus needed for effective client care.
These productivity boosts don’t just benefit clinicians – they also contribute to better outcomes for the entire organization.
Improved Organizational Performance
The ripple effect of improved clinician efficiency is felt throughout the organization. Faster note completion means clinicians can see more clients daily. For a mid-sized practice, this increased capacity can result in hundreds of thousands of dollars in extra revenue annually.
Integrated documentation and billing systems further enhance operations. Features like automated coding suggestions and compliance checks reduce claim denials and speed up reimbursements. With “Golden Thread” documentation – where assessments, treatment plans, and progress notes are clearly linked – organizations are better prepared for audits. Multi-site organizations, in particular, benefit from consolidated revenue cycle reporting, which simplifies the process of identifying and resolving billing issues quickly.
Higher Quality Care and Client Outcomes
Efficient documentation systems also elevate the quality of care. When clinicians aren’t bogged down by paperwork, they can focus on building stronger therapeutic relationships. Studies show that therapist burnout can weaken the therapeutic alliance and reduce empathy during sessions.
Cloud-based systems provide real-time access to complete client histories, improving care coordination. Authorized providers can instantly view treatment plans, progress notes, and outcome measures, avoiding duplicated assessments and ensuring team alignment. Additionally, automated integration of tools like PHQ-9 and GAD-7 scores enables clinicians to quickly identify high-risk clients, allowing for earlier interventions. This seamless access to information supports better decision-making and, ultimately, better client outcomes.
Conclusion
The burden of documentation isn’t just a logistical hassle – it’s a challenge that impacts every corner of a behavioral health organization. When clinicians spend 13.5 hours per week on paperwork instead of focusing on client care, it drains resources, contributes to burnout, and diminishes the quality of care provided.
To tackle this, tools like Welligent, Part of ContinuumCloud, offers tailored solutions designed specifically for behavioral health needs. Unlike generic medical EHRs, these systems are built to support the unique demands of behavioral health, such as narrative-driven progress, managing multiple client relationships, and long-term care.
The benefits are hard to ignore. Behavioral health organizations using specialized EHR software have slashed note completion times from 10–12 minutes to under 3 minutes. Clinicians are reclaiming 1–2 hours daily, time they’d otherwise spend on after-hours charting. Even more impactful, 88% of providers say they feel more present during sessions when the documentation process is streamlined.
This shift highlights a key principle:
“Administrative friction isn’t inevitable. It’s a design choice. The right EHR reduces burden instead of adding it.” – The PIMSY Team
When documentation systems are designed to complement clinical workflows, everyone benefits. Clinicians can focus on building therapeutic relationships, compliance teams can maintain audit-ready records, billing departments face fewer claim denials, and, most importantly, clients receive the attentive care they deserve. Aligning documentation with clinical needs isn’t just efficient – it’s essential for delivering meaningful care.
FAQs
What should I look for in a behavioral health EHR to cut documentation time?
When evaluating options, prioritize features like customizable templates – these let you tailor documentation to fit your specific needs. Another time-saving tool to look for is the ability to pull patient-reported outcomes directly into notes, so you can focus more on care and less on paperwork. These features not only enhance efficiency but also help ensure your documentation stays consistent and thorough.
How can AI documentation tools stay HIPAA and 42 CFR Part 2 compliant?
For substance use disorder (SUD) treatment, these tools go a step further. They use role-based access to ensure only authorized personnel can access specific information, audit logging to document every interaction with sensitive data, and data segmentation to separate and protect confidential details.
On top of that, regular monitoring and updates allow these tools to stay aligned with evolving regulations. This ensures ongoing compliance while keeping sensitive patient information secure.



{kind=link}
{kind=link}
{kind=link}